 |
MSI // “Mantis Shrimp Implant” (colloquial; designation varies by vendor cluster)
Status: Non-catalogue, boutique-class cybernetic subsystem
Deployment count (est. 2088): <200 confirmed installs
Origin trace: Fragmented; earliest cohesive documentation appears in a 2074 Cairo-based applied study on West African close-proximity operative doctrine
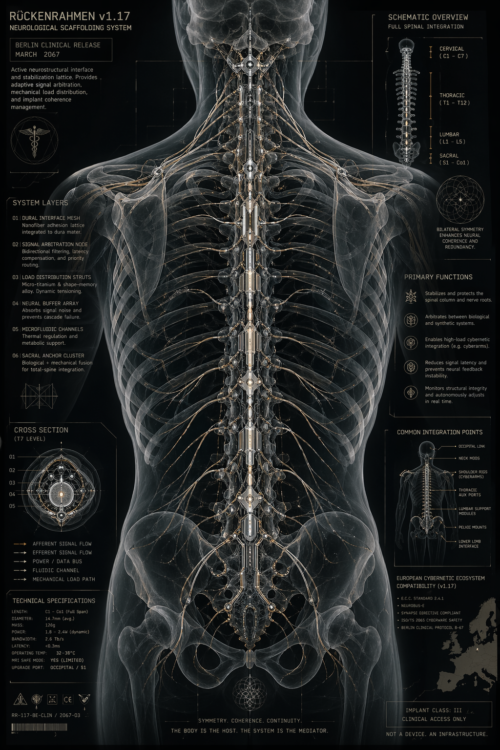
The MSI is not a discrete implant but a parametric kinetic deployment system integrated into existing thoracic cybernetic architecture. Each instance is individually CAD-CAM modeled against host-specific constraints: rib spacing, sternum geometry, existing scaffold implants (e.g. Rückenrahmen-class systems), power distribution topology, and neural arbitration layers. No two units are identical; even within a single vendor lineage, design drift is expected.
|

|
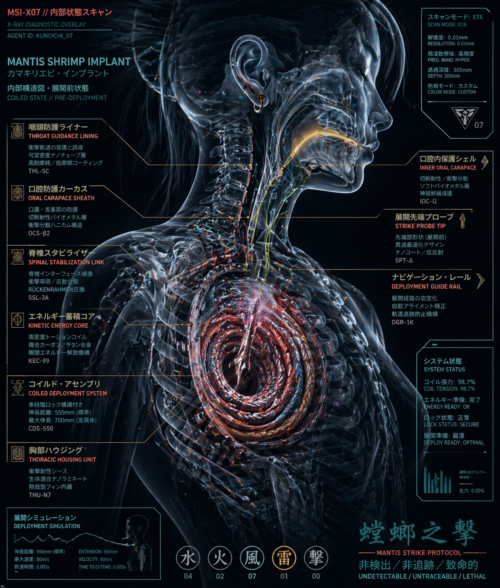
At its core, the MSI consists of a coiled acceleration spine—a segmented, pre-tensioned assembly housed within a reinforced thoracic cavity channel, typically parasternal or subclavicular. The structure is fabricated from high-elasticity metamaterials with layered fatigue resistance and embedded micro-actuation nodes. Energy storage is achieved through a hybridized system: mechanical preload (torsion/compression), supplemented by rapid-discharge capacitive bursts drawn from the host’s auxiliary power bus. The result is a high-velocity linear extension event with variable stroke length (standard: 40–55 cm; extended variants up to ~70 cm), deployable along a constrained vector determined at design time.
Control is mediated through the host’s neural interface, but notably not via direct conscious actuation in most builds. Instead, MSI units are typically slaved to a predictive targeting layer—a low-latency heuristic system that resolves spatial positioning, timing windows, and collision paths. This is necessary because raw human reaction time is insufficient to fully exploit the system’s acceleration profile. Integration with external targeting mods, tactical overlays, and motion prediction suites is strongly recommended; standalone operation degrades performance and increases risk of misalignment or structural rebound.
|
 |
The terminal assembly (“striker”) varies widely. Some configurations favor minimal cross-section and low observability, employing monomaterial tips with non-reflective, scan-resistant coatings designed to evade standard detection protocols. Others incorporate micro-sensing elements for positional feedback during extension/retraction cycles. All designs prioritize retraction reliability, as incomplete withdrawal introduces severe mechanical and physiological failure modes.
A defining constraint of the MSI is internal clearance and interference management. Deployment occurs within millisecond-scale windows but traverses a body that is already densely occupied by biological and artificial systems. As such, successful installations rely heavily on precomputed exclusion volumes and real-time arbitration with the host’s scaffolding systems. Rückenrahmen-class implants, when present, often act as a stabilizing backbone, absorbing recoil forces and redistributing load across the axial structure.
Thermal management is non-trivial. Rapid discharge events generate localized heat spikes along the acceleration spine; most builds incorporate microfluidic cooling loops tied into existing metabolic or implant cooling systems. Failure to dissipate heat effectively leads to material fatigue and increased maintenance intervals.
|

|
From a detection standpoint, MSI units are engineered for low signature presence. Housing materials are selected for reduced electromagnetic reflectivity and compatibility with common scan-noise profiles. However, complete invisibility is not achievable; high-resolution or invasive scanning will typically reveal anomalous structural densities
Maintenance requirements are high. The system undergoes extreme stress during each deployment cycle, necessitating periodic recalibration, component inspection, and, in some cases, partial reprinting of degraded segments. Field repair is not advised; most operators rely on specialized clinics with access to the original design parameters.
Operationally, the MSI is characterized by asymmetry: long periods of dormancy punctuated by extremely brief, high-intensity activation events. It is not a general-purpose augmentation but a situational tool, optimized for environments where proximity, timing, and concealment outweigh sustained engagement capability.
In summary, the MSI should be understood not as a weaponized appendage but as a kinetic subsystem embedded within the body’s infrastructure, whose effectiveness depends less on raw output and more on integration fidelity, predictive control, and the host’s tolerance for systemic complexity.
|